Written by: Robyn Otty, OTD, OTR/L, BCPR, FAOTA
June represents Alzheimer’s Disease (AD) awareness month and serves as a reminder how the disease impacts the individuals with AD and the loved ones affected by it. As a daughter who is directly touched by AD, this month especially promotes my reflection on how important it is to recognize the occupational disruption associated to all individuals who are connected to Alzheimer’s Disease.
According to the Alzheimer’s Association (2024), an estimated 6.9 million Americans over the age of 65 are living with the disease and considered the seventh leading cause of death. Furthermore, it has been estimated the growth of the disease increased 140% between 2000 and 2021, with an anticipated trend of a rising mortality rate to increase to 13.8 million by 2060. AD is the most common dementia type that represents degenerative changes within the brain. Symptoms of AD include memory and language challenges, apathy, depression, communication difficulties, poor judgment, and behavioral changes. Later stages include difficulty with basic level activities of daily living independence and difficulty swallowing (Alzheimer’s Association, 2024). To date there is no cure for Alzheimer’s Disease and the focus on prevention and manage the disease are top research priorities.
Recent studies point to the build-up of plaque (including beta-amyloid and tau proteins) as a significant marker of AD. With the focus of these proteins in the brain has given birth to medications (aducanumab and lecanemab) that isolate the beta-amyloid protein by preventing increased density of this protein in the brain. While there have been advancements for medications to treat symptoms of the disease, none has been discovered to cure or stop AD progression.
One opportunity to reduce the likelihood is to self-examine risk factors. While risk factors don’t necessarily guarantee the onset of AD, it can reduce the risk of acquiring AD. Table 1.0 identifies risk factors that are related to acquiring dementia based on genetics (non-modifiable) and unhealthy behaviors or treatable conditions (modifiable).
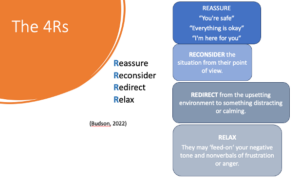 Without a cure, managing a person with AD’s symptoms can be challenging. Caregivers connected to individuals with Alzheimer’s Disease benefit from educational programming (Alzheimer’s Association, 2024). One model to manage someone diagnosed with AD is to use Budson’s (2022) 4R’s approach: Reassure, Reconsider, Redirect, and Relax. Using this acronym, the caregiver can provide statements of reassurance; always reconsider the point of view from someone with cognitive challenges (i.e. How would I feel if I could not understand the verbal directions?); redirect their attention to a more calming environment; and take deep breaths to minimize frustration or raising their voice. The visual, The 4Rs highlights the use of this approach.
Without a cure, managing a person with AD’s symptoms can be challenging. Caregivers connected to individuals with Alzheimer’s Disease benefit from educational programming (Alzheimer’s Association, 2024). One model to manage someone diagnosed with AD is to use Budson’s (2022) 4R’s approach: Reassure, Reconsider, Redirect, and Relax. Using this acronym, the caregiver can provide statements of reassurance; always reconsider the point of view from someone with cognitive challenges (i.e. How would I feel if I could not understand the verbal directions?); redirect their attention to a more calming environment; and take deep breaths to minimize frustration or raising their voice. The visual, The 4Rs highlights the use of this approach.

Caregivers can also provide opportunities for meaningful activity engagement. By providing self-care or leisure activities that are meaningful to the person with AD can support establishing a routine and decrease anxiety often seen with people with dementia (Green, 2024). Another intervention consideration is to examine the environment’s impact on the person’s behavior: Is the space overly stimulating from sensory point of view? Also, one may consider creating a more relaxed atmosphere or create an environment of safety, consider the use of music.
Finally, a specific “recipe” that guarantees management of any one person with AD does not exist. The medical practitioner should take the time to address their needs along with the surrounding caregivers’ wishes to create the ‘village of support’. Creating access for education can help the caregiver feel less isolated and more susceptible to caregiver fatigue. In the end, it ‘takes a village’ to create a meaningful and safe environment for a person with AD.
About Summit Professional Education
Summit equips Physical Therapists, Occupational Therapists and SLPs with better continuing education courses that provide CEUs while impacting patient outcomes. Find high-quality on-demand CE along with the largest offering of live options — including live webinars, live streams, and in-person courses. Want to deep dive on a topic? Summit offers hundreds of 6-hour courses for the most in-depth learning!
References:
Alzheimer’s Association. (2024). 2024 Alzheimer’s disease facts and figures. Alzheimer’s and Dementia The Journal of the Alzheimer’s Association, 20(5), 3708-3821. https://doi.org/10.1002/alz.13809
Green, M. (2024). Evidence connection- Occupation therapy interventions for older adults with Alzheimer’s disease and related dementias. American Journal of Occupational Therapy, 78, 7804390010. https://doi.org/10.5014/ajot.2024.050691
Sahathevan, R. (2014). Dementia: An overview of risk factors. In C.R. Martin & V. R. Preedy (Eds.) Diet and Nutrition in Dementia and Cognitive Decline (pp. 187-198). Elsevier Science & Technology.
Sousa, P. L., Krych, A. J., Cates, R. A., Levy, B. A., Stuart, M. J., & Dahm, D. L. (2017). Return to sport: Does excellent 6-month strength and function following ACL reconstruction predict midterm outcomes?. Knee surgery, sports traumatology, arthroscopy, 25(5), 1356-1363.